Why Ophthalmologists Recommend Corneal Cross-linking for Keratoconus

For a long time, treating keratoconus meant playing defense. A patient’s vision would blur, the prescription would change, and a few months later it would change again. Doctors could keep updating glasses and contacts, but they had no way to stop the cornea itself from getting worse.
Corneal cross-linking changed that, as it was the first treatment to address the disease at its source rather than chase symptoms, and that is the main reason ophthalmologists now recommend it so consistently. Keep reading to learn more about what cross-linking does and why timing matters so much for keratoconus patients.
Why Is Keratoconus Called a Progressive Disease?

The cornea is the clear, dome-shaped front surface of the eye, and in a healthy eye, it holds a smooth, round curve that focuses light cleanly onto the retina. Keratoconus is called progressive because the curve does not stay put. The cornea gradually thins and weakens over time, and the normal pressure inside the eye pushes the softening tissue outward into a cone-like bulge that grows more pronounced as the months pass.
That ongoing change is what separates keratoconus from a stable refractive error. As the cornea keeps steepening, it scatters light instead of focusing it, and patients often notice increasing nearsightedness, irregular astigmatism that glasses struggle to correct, glare and halos around lights, and a prescription that seems to need updating constantly.
Left alone, the cornea can keep worsening for years, and in advanced cases it scars or thins to the point that a corneal transplant becomes the only option. That forward momentum is exactly what cross-linking is designed to stop.
How Does Corneal Cross-linking Strengthen the Cornea?
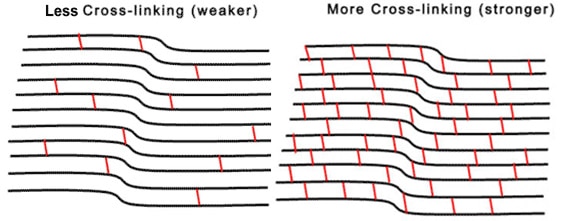
Corneal cross-linking, often shortened to CXL, works by reinforcing the cornea’s internal structure. The cornea is built largely from collagen fibers, and in keratoconus, the bonds holding those fibers together are too weak to keep the tissue rigid. Cross-linking adds new bonds.
The procedure uses two ingredients that work together. First, the surgeon applies riboflavin, which is vitamin B2, in eye-drop form so it soaks into the cornea. Then a controlled dose of ultraviolet light activates the riboflavin, triggering a reaction that creates fresh links between the collagen fibers. Those new connections stiffen and stabilize the cornea, much like adding cross-beams to a structure that was starting to sag. The result is a cornea far better able to hold its shape and resist further bulging.
Why Ophthalmologists Recommend Treating It Early
Cross-linking is the only FDA-approved treatment shown to halt the progression of keratoconus, and that fact alone explains much of why ophthalmologists favor it. CXL is the only widely available option that changes the trajectory of the disease instead of just managing its effects.
Cross-linking primarily aims to preserve and stabilize the cornea. A cornea that is stabilized while it is still relatively healthy gives a patient a far better long-term outcome than one treated after years of unchecked steepening and thinning.
Acting early also lowers the odds of reaching the advanced stage where a corneal transplant becomes necessary, a far more involved surgery with a much longer recovery.
When an ophthalmologist catches keratoconus in motion and recommends cross-linking, the goal is to lock in the cornea’s current condition before the disease has a chance to erode it further.
Does Cross-linking Improve Vision?
Patients are sometimes surprised to learn that cross-linking is not primarily a vision-sharpening procedure. Its main job is stabilization.
In some cases, patients may see improvement in vision as the cornea settles, but the central goal is to keep the condition from worsening rather than restoring crisp eyesight. That distinction shapes the rest of a patient’s care plan. Once the cornea is stable, several paths can sharpen vision from there.
For example, specialty contact lenses may be better able to vault over an irregular surface to deliver clearer focus. Cross-linking creates the stable foundation that makes those vision-correction options work better.
Who Is a Good Candidate for Corneal Cross-linking?
The best candidates are patients with early-stage keratoconus or corneal ectasia, a related condition in which the cornea thins and loses its regular shape. Catching the disease while it is still progressing but has not yet caused major damage is the ideal window. A history of certain corneal diseases or prior eye surgery can make someone ineligible, which is why a thorough evaluation matters before anything is scheduled.
What to Expect When You Visit Mueller Vision

A proper diagnosis starts with mapping the cornea. At Mueller Vision in Fort Worth, corneal topography produces a detailed contour map of the eye’s surface, which lets the team confirm keratoconus and, just as importantly, track whether it is actively progressing. That information drives the recommendation, because progression is the trigger for treatment.
The procedure itself is straightforward. Cross-linking is performed on an outpatient basis and usually takes less than an hour. The eye is numbed with anesthetic drops, the riboflavin solution is applied, and the ultraviolet light is then directed at the cornea for a set period to complete the cross-linking.
Dr. Brett Mueller, a board-certified and fellowship-trained ophthalmologist, evaluates each patient individually to determine whether cross-linking is the right move or whether another approach fits better. For keratoconus, getting in front of the disease early is the single most valuable thing a patient can do.
Wondering whether corneal cross-linking could be right for you? Schedule an appointment at Mueller Vision in Fort Worth, TX.






